Medicine For the Mind: Psychedelics For Depression & Mental Illness
How the new era of psychedelic medicine is challenging the conventional model of depression — for the better. 🌧🍄🌈


The current model for treating depression is broken. Depression levels continue to rise despite decades of antidepressant drug development.
Depression levels reached an all-time high in 2021, and today, nearly 1 in 3 people are affected by the condition.
New research in psychedelics suggests we’re looking at it all wrong — that depression isn’t merely a ‘dysfunction’ of the brain but something else buried deep within the psyche.
Here, we’ll explore what makes psychedelics so powerful for treating depression and how they’re changing our fundamental understanding of what causes this debilitating condition.
First of All, What is Depression?
Depression is a mood disorder that results in feelings of sadness, hopelessness, and loss of interest in things that would normally bring someone pleasure.
Types of Depression (According to the DSM-V)
- Persistent Depressive Disorder (PDD) — feelings of depression on most days for two years or longer. Previously referred to as dysthymia.
- Major Depressive Disorder — in addition to dysthymia, excessive feelings of guilt and suicidal ideation, and social isolation.
- Bipolar Disorder — periods of abnormally elevated mood followed by periods of abnormally depressed mood.
- Postpartum Depression (PPD) — depression that begins during or immediately following pregnancy.
- Premenstrual Dysphoric Disorder (PMDD) — significant feelings of depression during the premenstrual phase of a woman’s reproductive cycle.
- Seasonal Affective Disorder (SAD) — disturbances in circadian rhythm and vitamin D deficiency causing depression. Common in the dark winter months of northern latitudes.
- Atypical Depression — manifestation of depression that doesn’t fit the ‘typical’ presentation of the disorder.
- Adjustment Disorder (Depression Variant) — grief due to loss of any kind.
- Secondary Depression — depression caused by underlying medical disorders (such as Cushing’s disease or hypothyroidism).
- Disruptive Mood Dysregulation Disorder (DMDD) — characterized by severe and recurrent temper outbursts that are out of proportion to the situation.
- Premenstrual Dysphoric Disorder (PMDD) — a severe form of premenstrual syndrome (PMS) and can cause significant distress and interference with daily life.
What Causes Depression?
Depression is a symptom, not a disease unto itself. All forms of depression have an underlying cause — some are much more difficult to identify than others.
The causes of depression can be broken down into two categories:

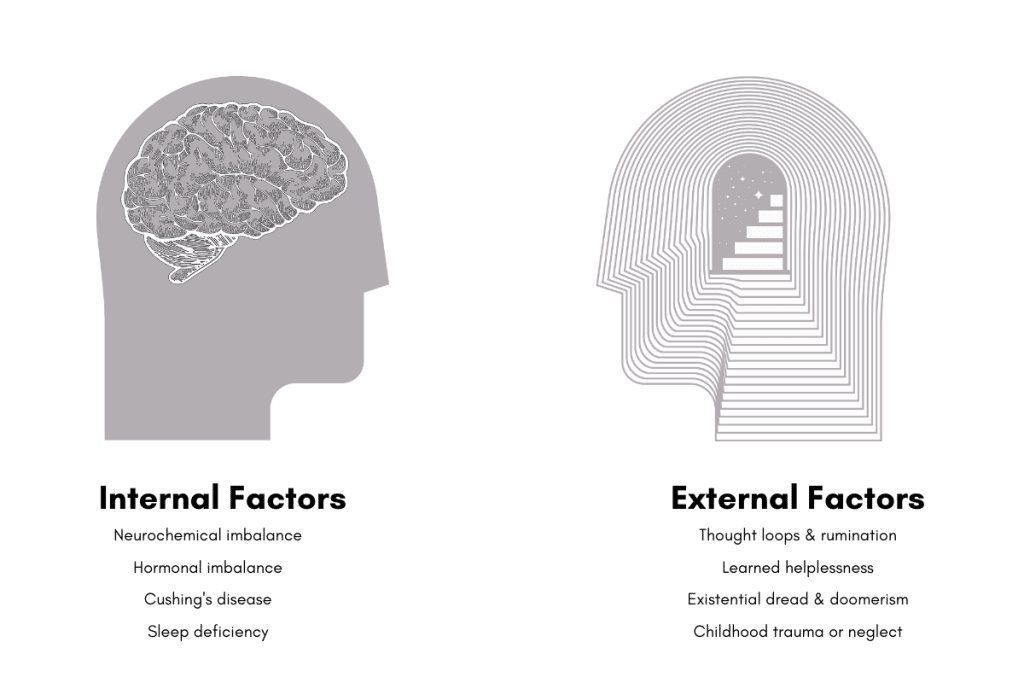
1. Internal & Chemical Causes of Depression
Chemical causes originate from within the system. This can include hormone imbalance, side effects from medications or illicit substances, or so-called ‘chemical imbalances.’
Some conditions can cause depression as a side effect, such as Cushing’s disease, hypothyroidism, sleep disorders, and chronic pain.
Treatment for chemical or internal depression involves altering brain chemistry with antidepressants. These medications are designed to boost neurotransmitters and induce positive emotions in depressed individuals.
Unfortunately, these medications do little to treat the underlying cause. When people stop taking antidepressants they often slip right back into the condition within a few weeks or months.
2. External Causes of Depression
Researchers are now discovering that the true cause of depression for most people goes beyond our physical hardware (the brain). Studies have shown that any changes in how we think can manifest in real, measurable changes in brain chemistry and mood.
So what kind of thought patterns cause depression?
Well, there are many.
Examples of external causes of depression:
- Thought loops & rumination — continuously thinking the same thoughts, which tend to be dark, sad, or disturbing in nature.
- Learned helplessness — the belief that we’re powerless to solve our problems.
- Existential dread — questioning of whether or not one’s life has purpose, meaning, or value.
- Doomerism — stems from the overwhelming immensity of global problems like overpopulation, climate change, and the possibility these events will result in the annihilation of the human species.
- Childhood trauma or neglect — traumatic experiences as a child cause us to disconnect with the self as a form of self-preservation. This disconnection remains until there’s a conscious effort to restore it.
Most of the time, we’re unaware of the limiting or negative thought patterns that exist in our minds.
Symptoms that may appear to be “chemical” in nature, actually originate from thoughts outside our conscious awareness.

Modalities like psychedelic-assisted therapy and shadow work are centered around surfacing these negative unconscious thoughts and patterns into the sphere of conscious awareness in order to rewrite them.
Psychedelics For Depression: How Does It Work?
Psychedelics themselves don’t cure depression. The real cure comes from the deep, personal insights gained during the experience. These insights change the way we think (unconsciously), which permeates into higher cognitive centers and alters our brain chemistry.
This explains why psychedelics are so effective at treating depression after just a single session — compared to the weeks, months, or years needed with chemical antidepressants.
Treating depression requires a fundamental shift in ontology rather than a simulated emotional buttress through antidepressant drugs.
Here are six of the leading theories and research on how psychedelics work for depression. We’ll explore both internal (chemical) and external (metaphysical) mechanisms.
1. Psychedelics Suppress the Default Mode Network (DMN)
The DMN (default mode network) is one of the seven large-scale brain networks. It’s the group’s ringleader, tasked with keeping the other brain networks in order.
The DMN develops in early childhood. As it develops, our thoughts become more rigid and efficient.
The actions of the DMN give humans a key advantage over other animals in how we process information. It allows us to carry out complex tasks and apply abstract concepts like remembering the past or anticipating the future.
However, excessive DMN activity can also lead to more cognitive rigidity — which is considered one of the primary external causes of depression and anxiety.
Too much rigidity in our thinking can lead to an enclosed and biased perspective of the world beyond our fixed assumptions and beliefs. Rumination and learned helplessness are direct byproducts of this.
Classical psychedelics (such as LSD, DMT, or psilocybin) can temporarily suppress the default mode network. While offline, the DMN no longer restrains the other brain networks, leading to higher entropy and chaos, which correspond to the psychedelic experience itself.
However, psychedelics only suppress the DMN for a few hours. Eventually, these substances wear off.
Early research on this phenomenon suggests that when the DMN comes back online, it behaves differently than it did before taking psychedelics. Physical changes such as blood flow and functional connectivity are well documented following treatments with LSD and psilocybin.
Psychedelics appear to facilitate a hard reset of our default mode network — reducing its control over the other brain networks.
The long-term effects of DMN suppression align with the personality trait “openness” — which involves increased imagination and creativity, enhanced tolerance of others’ viewpoints and values, aesthetic appreciation, and empathy.
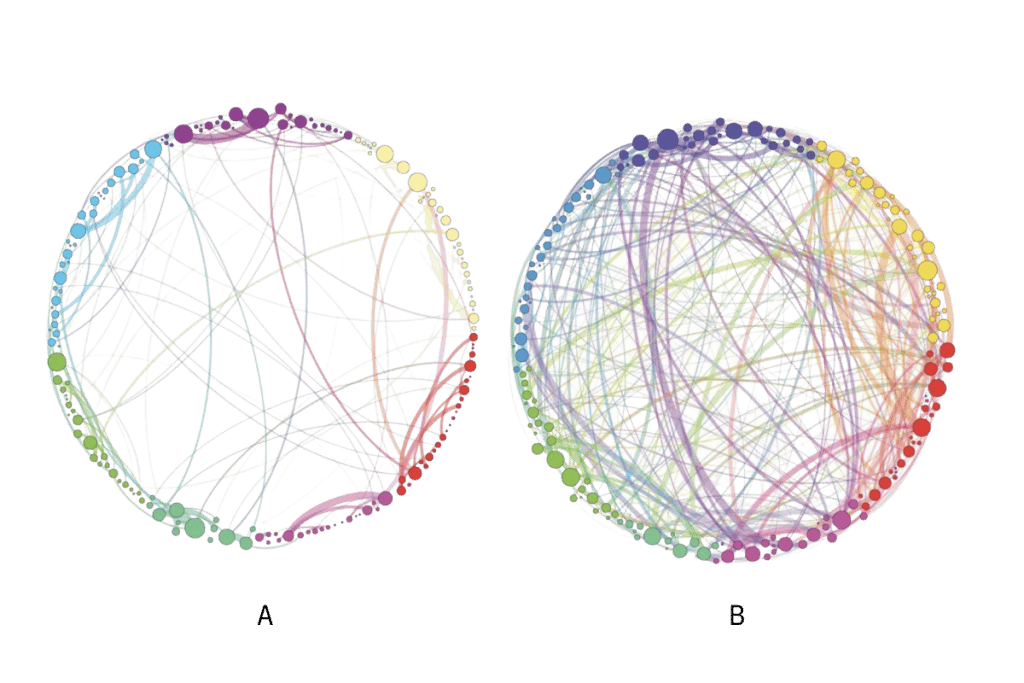
Source: Petri et al., 2014
DMN & Patterns of Rumination
One of the consequences of the DMN is rumination and negative thought loops.
A recent online survey (2021) examined how psychedelics alter thought patterns and what impact these changes had on depression, anxiety, and stress [2].
Researchers noted a significant decrease in rumination patterns and increased self-reflection and compassion following the psychedelic experience.
- Rumination refers to negative self-focus motivated by the perception of threats, self-harm, and injustice. Self-rumination has a high correlation with depression [5].
- Self-reflection refers to the process of observing and evaluating their own emotional, behavioral, and cognitive processes. Self-reflection has a high correlation with contentment and well-being.
People who spend more time self-ruminating over past events, perceived inadequacies, or unrealistic desires have a snowball effect. This practice can lead to a lack of sleep, social isolation, missed opportunities, poor diet, and lifestyle habits, or the development of an obsession, fixation, or addiction as a source of distraction.
Likewise, if we spend more time in self-reflection, the snowball rolls in the other direction — leading to higher energy levels, increased sociability, maintenance of healthy habits, and a greater sense of happiness and contention. This, in turn, makes it easier to remain in a state of positive self-reflection.
2. Psychedelics Can Occasion Mystical Experiences
Mystical or “peak” experiences are characterized by feelings of deep spiritual, existential, transformative, and transpersonal awareness.
These experiences often result in insights that lead to a distinct shift in one’s ontological position of the world.
Studies have shown that up to 86% of people who have used psychedelics in a therapeutic setting claim the experience to be within the top five most meaningful experiences of their lifetime [13].
Common themes of mystical experiences include:
- Encounters with “supernatural” beings
- Comprehension of spacial and temporal vastness
- Experiences of an “ultimate reality”
- A sense that all things are connected (unitive experience, non-dual states)
Changes in Metaphysical Beliefs: Non-Physicalist Beliefs
Mystical experiences have also been shown to alter one’s metaphysical position.
Most people hold distinct metaphysical positions even if they aren’t aware of it [3]. These positions affect every aspect of one’s existence, including our mental health, motivation, decision-making, and personal well-being.
Some of these belief systems limit our capacity to find meaning in life and understand the purpose and pain of existence.
Of particular importance are the positions of physicalism (materialism), idealism, and dualism:
- Physicalism (materialism) — the belief that the nature of reality is purely physical, and there is nothing beyond the physical realm.
- Idealism — the belief that all physical properties are derived from a non-physical (mental) reality.
- Dualism — the belief that the nature of reality consists of both physical and mental influence.
A recent study found that after taking psilocybin, participants displayed a shift away from hard materialism (survey) towards more dualistic beliefs [4]. Researchers also observed a positive correlation between non-physicalistic beliefs and a greater sense of wellbeing.
This was verified in another clinical trial that compared the effects of psilocybin against conventional antidepressant therapy (a 6-week course of escitalopram). The study examined the capacity of each treatment for inducing positive metaphysical position changes [7]. Only the psilocybin group resulted in significant changes in worldview.

3. Psychedelics Uncover Unconscious Influences: The Shadow
Psychedelics are considered a valuable tool for uncovering traits we deem “undesirable” and how our attempts to suppress them only make them stronger.
This is the fundamental principle behind a form of therapy called shadow work — which seeks to reintegrate ‘negative’ traits such as grief that reside in our unconscious. The goal of this practice is to reduce their influence over our thoughts and emotions.
The concept of the shadow was coined by Dr. Carl Gustav Jung. He was a student of Sigmund Freud and one of the most influential psychologists to have ever lived. His ideas were well ahead of his time but are starting to resurface in psychology today.
The shadow describes the unconscious, suppressed aspects of the self. It’s the traits we either don’t like about ourselves or believe others in society won’t like — such as grief, lust, rage, or jealousy.
The idea is that the more we deny and suppress these feelings (all of which are completely natural and out of our control), the stronger they become.
When talking about depression, grief is one of the main traits to consider. Grief is an emotional, physical, and philosophical response to loss. It’s completely natural and not something that can be suppressed or avoided.
When we try to suppress grief, we push it deeper into our unconscious mind. Here, grief maintains its influence on how we feel and act — but we’re no longer aware of how this influence manifests in our conscious thoughts and emotions.
Acknowledging grief and other aspects of the shadow means accepting them for what they are, inviting them into the conscious sphere of awareness, and leveraging them as a strength rather than a weakness.
Here are some of the changes that can happen when we learn to integrate our shadow:
- Grief facilitates connection with the self & others
- Fear becomes a source of courage
- Aggression becomes a source of passion
- Pain becomes a lesson in perseverance & grit
- Selfishness becomes a lesson in empathy
- Lust facilitates passion, connection, & love
Related: 100 Journal Prompts For Shadow Work & Psychedelic Integration
4. Psychedelics Temporarily Increase Suggestibility
Psychedelics have been shown to enhance suggestibility from both the therapist conducting the session [10,11], as well as other members of the group during communal psychedelic ceremonies [12].
This effect is important in treating mental health conditions because it may make the patient more responsive and engaged with the positive suggestions of the therapist.

5. Psychedelics Cause Neurochemical Changes & Neuroplasticity
Research supports the idea that psychedelics induce or enhance neuroplasticity [15]. But what is neuroplasticity, and why is it relevant for treating depression?
Neuroplasticity is a measurement of a neuron’s capacity to grow and change. It’s relevant in the discussion of depression because a disruption in neuroplasticity is thought to be a key factor in the underlying mechanisms of depressive disorders [20].
Many of the factors that contribute to the pathophysiology of depression also disrupt neuroplasticity — such as traumatic events, sleep deficiency, and chronic stress.
The negative effects of stress on neuroplasticity include:
- Impairs hippocampus-dependent memory [21].
- Decreases neuronal dendrite branching in the hippocampus [22].
- Increases corticosteroid levels and downregulates hippocampal neurogenesis [23].
While in a neuroplastic state, both the individual neurons and the entire system are subject to being remapped [17,19]. This process facilitates the optimization of neural pathways and may increase cognitive flexibility.
A few different kinds of psychedelics have been reported to facilitate neuroplasticity — including serotonergic psychedelics like LSD, psilocybin, and DMT. These effects largely rely on the interaction with Sigma-1 receptors, 5HT2A receptors, and BDNF.
Even conventional SSRI medications have been suggested to work by enhancing neuroplasticity in the brain [18], rather than relying solely on increasing synaptic serotonin levels.
Non-serotonergic psychedelics have been shown to also have this effect, such as ketamine [16] — which is already one of the most common psychedelic medicines used in treating depression in the clinical setting.
6. Psychedelics May Alter Cerebral Blood Flow
One of the older theories that’s been partially debunked in the last couple of years is the idea that psychedelics work by increasing blood flow to the brain.
fMRI machines have proven that while some areas of the brain may experience increased blood flow, the opposite tends to occur as well — especially in key regions of the neocortex.
For example, research has shown that psilocybin causes a decrease in blood flow to the amygdala and temporal cortex [1].
The amygdala is associated with the fear-response and directly correlates with depression [8]. A reduction of blood flow to this brain region implies a suppressive action from psychedelics.
Likewise, a reduction in blood flow to the temporal cortex is thought to be directly correlated with psilocybin’s ability to suppress the default mode network — which is one of the other leading theories for how psychedelics treat depression.
Current Research: Psychedelics & Depression
The concept of using psychedelics for treating mental health diseases isn’t new — humans have been using these substances for thousands of years for ceremonial, spiritual, and medicinal purposes.
Modern scientific research first began examining the effects of psychedelics in the 1940s but didn’t pick up until the 1960s. Research peaked around 1962, just before the Harvard Psilocybin Project fired its lead researchers, Timothy Leary and Richard Alpert, and shut down the program.
Unfortunately, in 1968, right when psychedelic research was at its peak, the US government, followed by numerous governments all around the world, banned this research. The ban lasted about 32 years before it was permitted for research purposes in 2000.
Today, research has picked up where researchers from decades earlier left off — and the results have been nothing short of incredible.
1. Psilocybin For Depression
There are numerous studies exploring the effects of psilocybin (the active ingredient in magic mushrooms) on mental health diseases — including depression.
Psilocybin acts as a serotonergic psychedelic — facilitating mystical and transformative experiences, enhancing suggestibility, and inducing neuroplasticity.

So far, the results we’re seeing from psilocybin research blow everything else out of the water. The success rates from just one session of psilocybin (when used in the proper context and with the right guidance) result in a more significant reduction of depressive symptoms than conventional antidepressant medications taken over several weeks or months.
Psilocybin Research Matrix: Depression
| Author, Year | Level of Evidence | Study Size | Results (Study Findings) | Treatment (Dose) |
| Davis et al., 2021 | RCT | 27 | 71% of patients had a reduction in depression scores by over 50% at the 4-week follow-up. 54% were in complete remission. | Two psilocybin sessions (20 mg/70 kg and 30 mg/70 kg) separated 8 weeks apart |
| Carhart-Harris et al., 2017 | Case-Control Study | 19 | Decreased depressive symptoms were observed in all 19 patients | Two psilocybin doses (10 mg followed by 25 mg, 7 days apart) |
| Carhart-Harris et al., 2016 | Open-Label Study | 12 | Persistent decrease in depressive symptoms and sustained improvements in anhedonia | Two psilocybin doses (10 mg and 25 mg, 7 days apart) |
| Griffiths et al., 2016 | RCT | 51 | Significant reduction in depression and anxiety scores after 6 months in 80% of study participants | Three psilocybin doses separated by 5 weeks each (very low (placebo-like) dose, moderate dose (1 or 3 mg/70 kg), and high dose (22 or 30 mg/70 kg) |
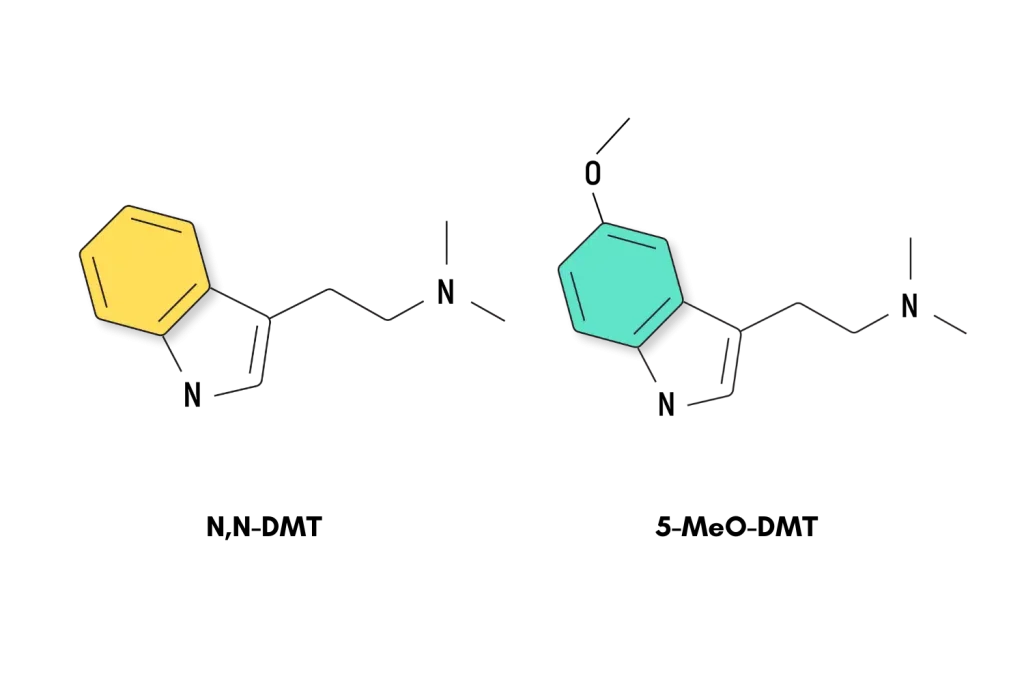
2. DMT & Ayahuasca For Depression
DMT (dimethyltryptamine) is one of the most powerful, yet short-lived psychedelics on Earth.
The power of DMT for healing depression lies in its reliability for inducing powerful mystical experiences.
Its short duration (20–45 minutes) is advantageous over other psychedelics within the clinical setting too. It’s much easier for a therapist to administer a DMT session over the course of about an hour, rather than having to dedicate 6–10 hours for a single session with magic mushrooms or LSD.
This doesn’t apply to ayahuasca, a traditional plant medicine consisting of the ayahuasca vine (Banisteriopsis caapi) and a natural source of DMT (such as Mimosa pudica or Psychotria viridis). Ayahuasca ceremonies can last up to 12 hours and require the skill of a trained shaman.
Ayahuasca brings additional facets to the table that make it especially useful for the purposes of treating mental health.
- The rituals associated with ayahuasca may make participants even more open to suggestibility during and after the session
- The group model of ayahuasca ceremonies provide additional layers of support
- Ayahuasca contains other medicinal ingredients, such as various harmala alkaloids (MAO inhibitors)
- The methods for administering ayahuasca consider other aspects of ones mental and physical health (the psychoactive dose of ayahuasca is just one component of the medicine)
Another traditional form of DMT therapy is the venom of the Bufo alvarius toad — which contains high concentrations of 5-MeO-DMT and bufotenin. The venom from the toad is usually smoked or vaped, producing immediate effects.
Due to concerns over ecological damage from harvesting bufo toad venom, many experts are calling for the use of synthetic 5-MeO-DMT instead, which produces effects that are indistinguishable from the real thing.
DMT & Ayahuasca Research Matrix: Depression
| Author, Year | Level of Evidence | Study Size | Results (Study Findings) | Treatment (Dose) |
| Osório et al., 2015 | Open-Label Study | 6 | Reductions in depression scores up to 82% following the treatment | 1 ayahuasca ceremony |
| Palhano-Fontes et al., 2019 | RCT | 29 | Significant reduction in depression scores in the ayahuasca group compared to the control | A single dose of either ayahuasca or placebo |
| Sanches et al., 2016 | Open-Label Study | 17 | Significant decreases in HAM-D, MADRS, and anxious-depression BPRS subscale scores were observed from days 1–21 following treatment | A single dose of 120 to 200 mL of ayahuasca (2.2 ml/kg) (96 to 160 mg DMT and 25 to 42 mg harmine) |
| Davis et al., 2019 | Survey | 362 | 80% of participants who self-reported a history of depression reported clear improvements in depression symptoms following 5-MeO-DMTuse | One or more 5-MeO-DMT sessions |
3. Ketamine For Depression
Ketamine is unlike any antidepressant on the market today. It doesn’t target serotonin as SSRIs do, and it doesn’t induce mystical states like psilocybin, DMT, or LSD.
So how does it work?
Ketamine is classified as a dissociative, which refers to its ability to dissociate the user from their body and mind. Users feel as though they’re somewhere else and lose their sense of connection with the self.
While this experience is distinctly different from other psychedelics and isn’t as reliable for inducing mystical experiences, this hallucinogenic state is still considered useful in altering fixed beliefs or patterns that contribute to depression.
Where ketamine shines is in its ability to stimulate synaptic plasticity in the brain [25].
Ketamine therapy is a proven treatment for depression, known for producing rapid results. Just one 40-minute IV therapy has an average success rate of around 60%.
The only problem is that these effects tend to wear off 7–14 days later. Users need an average of around six sessions for longer-lasting results, and many still need to come back to ketamine therapy 6–12 months later.
Ketamine Research Matrix: Depression
| Author, Year | Level of Evidence | Study Size | Results (Study Findings) | Treatment (Dose) |
| Lally et al., 2014 | RCT | 36 | Rapid and significant reduction in anhedonia after a single ketamine infusion lasting up to 14 days | IV ketamine hydrochloride (0.5 mg kg) and placebo (dosed 2 weeks apart) in randomized order |
| Szymkowicz et al., 2013 | Open-Label Study | 3 | Rapid and significant reduction in depression scores after 5 treatments | IV ketamine (0.5 mg/kg) |
| Murrough et al., 2013 | Open-Label Study | 24 | Significant reduction in depression symptoms in 70.8% of participants | Six doses of IV ketamine (0.5 mg/kg) three times per week |
| Ibrahim et al., 2012 | Open-Label Study | 42 | Significant reduction in depression symptoms in 62% of participants lasting up to 4 weeks | Single-dose of IV ketamine (0.5 mg/kg) followed by either riluzole (100–200 mg/day) or placebo for 4 weeks |
| Murrough et al., 2013 | RCT | 73 | Rapid and significant reduction in depression scores following a single treatment (64%) | Randomized treatment of a single dose of IV ketamine or midazolam control |
Psychedelic-Assisted Psychotherapy is Revolutionizing Healthcare
We’re on the brink of a revolution in the way we treat mental health as a society.
Evidence for the usefulness of psychedelics in mental health becomes stronger every day, and new bills are moving through the legal system that seeks to legalize psychedelic-assisted psychotherapy.
Psilocybin therapy is already available for terminal patients living in Canada and Oregon, and a protocol for using MDMA in the treatment of PTSD is currently awaiting approval by the FDA.
We could see psychedelics become a core component of how we treat depression and other mental health disorders by the end of the decade.
However, there are some ethical hurdles to get through before we get there.
The Downsides of Commercialized Psychedelic Medicine
One of the most concerning aspects of legalizing and commercializing psychedelics is the emergence of companies entering the space to make a quick profit — often at the expense of the patient.
Companies seeking to commercialize psychedelic medicine are inflating the cost of treatments and fail to incorporate critical components of the healing process — such as integration of the experience. There are already dozens of ketamine clinics that operate more like a business than a source of healing. Patients enter, get plugged into an IV, and are left alone for 40 minutes. When it’s over, they’re rescheduled for another appointment and sent home.
Compass Pathways is another example seeking to monopolize psychedelic therapy. The company was recently granted a patent on their new crystalline psilocybin. This way, the company can apply for FDA approvals using a patented compound rather than generic psilocybin. If approved, Compass Pathways can charge whatever they want for the treatment.
While there’s a case to be made that pure, concentrated psychedelics are useful in a clinical setting because it ensures consistency between doses, branded molecules drive up the cost of treatment substantially.
Luckily, there are plenty of alternatives far too old for a company to patent these days — such as 4-AcO-DMT (prodrug of psilocin) and LSD. However, because of this lack of patentability, there isn’t much of a push to bring these molecules into the clinic.
Key Takeaways: Can Psychedelics Help With Depression?
So far, the research backing the use of psychedelics for treating depression is promising, to say the least. There have already been several clinical studies proving these substances offer clear therapeutic benefits in ways we’re only just beginning to understand.
What makes psychedelics so useful for treating mental health disorders is their capacity to treat beyond the physical components of the brain (neurons, neurotransmitters, blood flow, etc.) and address underlying dysfunctions residing in the mind.
While the research has been promising — strong enough for the FDA to declare compounds like psilocybin a “breakthrough therapy” — we still have a long way to go, and there’s plenty we still don’t understand.
Stay up to date as new research in the field of psychedelics emerges by subscribing to our monthly newsletter below.
References
- Carhart-Harris, R. L., Roseman, L., Bolstridge, M., Demetriou, L., Pannekoek, J. N., Wall, M. B., … & Leech, R. (2017). Psilocybin for treatment-resistant depression: fMRI-measured brain mechanisms. Scientific reports, 7(1), 1-11.
- Fauvel, B., Strika-Bruneau, L., & Piolino, P. (2021). Changes in self-rumination and self-compassion mediate the effect of psychedelic experiences on decreases in depression, anxiety, and stress. Psychology of Consciousness: Theory, Research, and Practice.
- Paulhus, D. L., & Carey, J. M. (2011). The FAD–Plus: Measuring lay beliefs regarding free will and related constructs. Journal of personality assessment, 93(1), 96-104.
- Timmermann, C., Kettner, H., Letheby, C., Roseman, L., Rosas, F. E., & Carhart-Harris, R. L. (2021). Psychedelics alter metaphysical beliefs. Scientific reports, 11(1), 1-13.
- Alderman, B. L., Olson, R. L., Bates, M. E., Selby, E. A., Buckman, J. F., Brush, C. J., … & Shors, T. J. (2015). Rumination in major depressive disorder is associated with impaired neural activation during conflict monitoring. Frontiers in human neuroscience, 9, 269.
- Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry, 62(6), 593-602.
- Carhart-Harris, R., Giribaldi, B., Watts, R., Baker-Jones, M., Murphy-Beiner, A., Murphy, R., … & Nutt, D. J. (2021). Trial of psilocybin versus escitalopram for depression. New England Journal of Medicine, 384(15), 1402-1411.
- Hamilton, J. P., Siemer, M., & Gotlib, I. H. (2008). Amygdala volume in major depressive disorder: a meta-analysis of magnetic resonance imaging studies. Molecular psychiatry, 13(11), 993-1000.
- Hartogsohn, I. (2018). The meaning-enhancing properties of psychedelics and their mediator role in psychedelic therapy, spirituality, and creativity. Frontiers in neuroscience, 12, 129.
- Carhart-Harris, R. L., Kaelen, M., Whalley, M. G., Bolstridge, M., Feilding, A., & Nutt, D. J. (2015). LSD enhances suggestibility in healthy volunteers. Psychopharmacology, 232(4), 785-794.
- Studerus, E., Gamma, A., Kometer, M., & Vollenweider, F. X. (2012). Prediction of psilocybin response in healthy volunteers. PloS one, 7(2), e30800.
- Haijen, E. C., Kaelen, M., Roseman, L., Timmermann, C., Kettner, H., Russ, S., … & Carhart-Harris, R. L. (2018). Predicting responses to psychedelics: a prospective study. Frontiers in pharmacology, 9, 897.
- Griffiths, R. R., Richards, W. A., McCann, U., & Jesse, R. (2006). Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology, 187(3), 268-283.
- Herzog, R., Mediano, P. A., Rosas, F. E., Carhart-Harris, R., Perl, Y. S., Tagliazucchi, E., & Cofre, R. (2020). A mechanistic model of the neural entropy increase elicited by psychedelic drugs. Scientific reports, 10(1), 1-12.
- De Vos, C. M., Mason, N. L., & Kuypers, K. P. (2021). Psychedelics and Neuroplasticity: A Systematic Review Unraveling the Biological Underpinnings of Psychedelics. Frontiers in Psychiatry, 1575.
- Lepack, A. E., Bang, E., Lee, B., Dwyer, J. M., & Duman, R. S. (2016). Fast-acting antidepressants rapidly stimulate ERK signaling and BDNF release in primary neuronal cultures. Neuropharmacology, 111, 242-252.
- Kourrich, S., Su, T. P., Fujimoto, M., & Bonci, A. (2012). The sigma-1 receptor: roles in neuronal plasticity and disease. Trends in neurosciences, 35(12), 762-771.
- Yagasaki, Y., Numakawa, T., Kumamaru, E., Hayashi, T., Su, T. P., & Kunugi, H. (2006). Chronic antidepressants potentiate via sigma-1 receptors the brain-derived neurotrophic factor-induced signaling for glutamate release. Journal of Biological Chemistry, 281(18), 12941-12949.
- Kurrasch‐Orbaugh, D. M., Parrish, J. C., Watts, V. J., & Nichols, D. E. (2003). A complex signaling cascade links the serotonin2A receptor to phospholipase A2 activation: the involvement of MAP kinases. Journal of neurochemistry, 86(4), 980-991.
- Liu, W., Ge, T., Leng, Y., Pan, Z., Fan, J., Yang, W., & Cui, R. (2017). The role of neural plasticity in depression: from hippocampus to prefrontal cortex. Neural plasticity.
- Pittenger, C., & Duman, R. S. (2008). Stress, depression, and neuroplasticity: a convergence of mechanisms. Neuropsychopharmacology, 33(1), 88-109.
- Son, H., Banasr, M., Choi, M., Chae, S. Y., Licznerski, P., Lee, B., … & Duman, R. S. (2012). Neuritin produces antidepressant actions and blocks the neuronal and behavioral deficits caused by chronic stress. Proceedings of the National Academy of Sciences, 109(28), 11378-11383.
- Masi, G., & Brovedani, P. (2011). The hippocampus, neurotrophic factors and depression. CNS drugs, 25(11), 913-931.
- Petri, G., Expert, P., Turkheimer, F., Carhart-Harris, R., Nutt, D., Hellyer, P. J., & Vaccarino, F. (2014). Homological scaffolds of brain functional networks. Journal of The Royal Society Interface, 11(101), 20140873.
- Kavalali, E. T., & Monteggia, L. M. (2012). Synaptic mechanisms underlying rapid antidepressant action of ketamine. American Journal of Psychiatry, 169(11), 1150-1156.